
Understanding Multiple System Atrophy (MSA)
Multiple System Atrophy (MSA) is a rare and progressive neurodegenerative disorder that falls under the category of atypical parkinsonian syndromes. While it shares some similarities with Parkinson’s disease (PD), MSA is a distinct condition that affects multiple systems in the body—making early recognition and management especially important.
What is Multiple System Atrophy?
MSA is characterized by a combination of:
Parkinsonism (slowness, stiffness, tremor)
Cerebellar dysfunction (coordination and balance issues)
Autonomic dysfunction (problems with blood pressure, bladder, bowel, and more)
At a cellular level, MSA involves the accumulation of abnormal proteins (Papp-Lantos bodies) within glial cells, which normally support and protect neurons. Over time, this leads to degeneration in key areas of the brain including the basal ganglia, cerebellum, and brainstem.
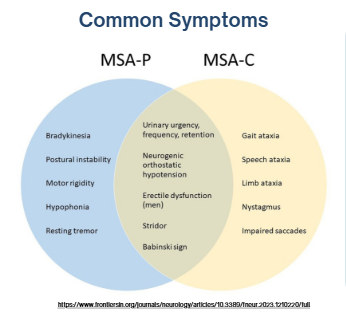
There are two primary types of MSA:
MSA-P (Parkinsonian type): Dominated by movement-related symptoms
MSA-C (Cerebellar type): Dominated by coordination and balance impairments
MSA vs. Parkinson’s Disease: What’s the Difference?
In its early stages, MSA is often mistaken for Parkinson’s disease. However, several key differences can help distinguish the two:
Disease progression: MSA progresses more rapidly than PD
Autonomic symptoms: Early issues like orthostatic hypotension, bladder dysfunction, and sexual dysfunction are common in MSA but less typical early in PD
Motor symptoms: Falls and coordination issues tend to appear earlier in MSA
Medication response: Individuals with MSA often show little to no improvement with levodopa, a common Parkinson’s medication
Pathology: While both involve alpha-synuclein, MSA affects multiple brain systems rather than primarily dopamine pathways
Common Symptoms of MSA
Symptoms vary depending on the type but often include:
Motor Symptoms
Bradykinesia (slowness of movement)
Muscle rigidity
Postural instability
Gait ataxia (uncoordinated walking)
Tremor (less common than in PD)
Autonomic Symptoms
Orthostatic hypotension (drop in blood pressure when standing)
Urinary urgency, retention, or incontinence
Constipation
Changes in sweating
Sexual dysfunction
Other Symptoms
Sleep disturbances (REM sleep behavior disorder, sleep apnea, stridor)
Speech difficulties
Emotional regulation challenges
One of the biggest challenges with MSA is that there is no single test to definitively diagnose it. Diagnosis is based on clinical presentation, medical history, and neurological evaluation.
Rehabilitation and Therapy: The Role of PT and OT
Although there is currently no cure for MSA, rehabilitation plays a critical role in maintaining quality of life.
The primary goals of physical and occupational therapy include:
Maintaining safety
Promoting independence
Preserving functional abilities
Key Therapy Interventions
Improving balance and reducing fall risk
Addressing postural instability and coordination deficits
Training safe transfers and movement strategies
Recommending appropriate mobility aids
Managing orthostatic hypotension during activity
Adapting daily activities (bathing, dressing, eating)
Supporting fine motor skills and hand function
Early and consistent therapy can help individuals stay active and engaged in daily life for as long as possible.
Final Thoughts
MSA is a complex and challenging condition—not only for those diagnosed, but also for their families and care teams. Increased awareness and early recognition are essential for appropriate management and support.
While the disease progresses, a proactive and multidisciplinary approach—including physical therapy, occupational therapy, and medical management—can make a meaningful difference in maintaining independence and quality of life.